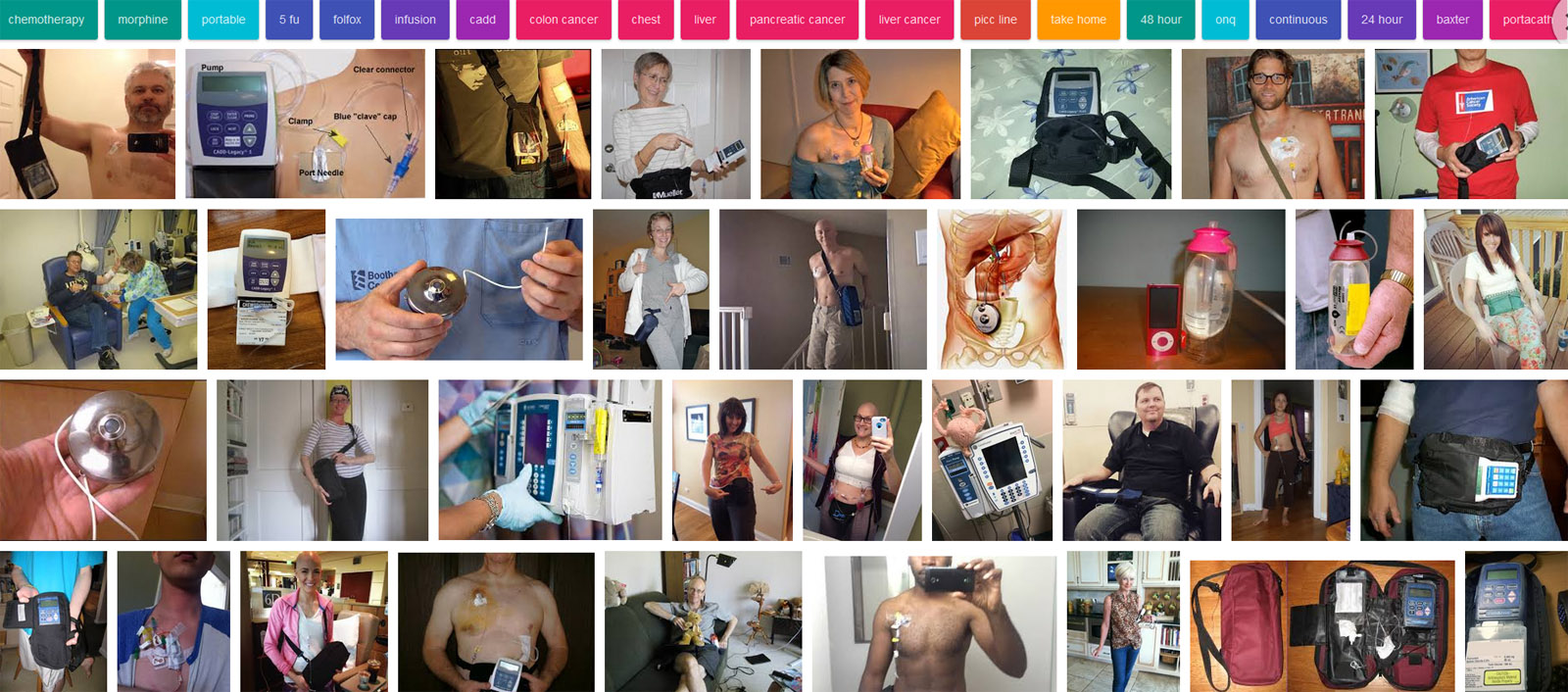
Google Images, screenshot.
It wasn’t long ago I was moaning about the size of the chemo pump I get to be tethered to for two days per session. My friend who is also undergoing treatment told me their pump was more like an old Walkman, and electric rather than gravity fed, like mine. It’s also flat, rather than the silly giant capsule shape of mine. The above barely begins to cover all the different types, that’s not close to the whole page. Which leads me to wonder about standardisation, patient care, and patient outcomes. Whether or not you are paying attention to it, obviously everything about treatment has its effect on you, and user friendliness counts on some level, I’m sure. Of course, capitalism reigns supreme here in Ustates, and it’s quite apparent that there are plenty of chemo pumps all vying for attention and purchase. Obviously, more prestigious institutions with money behind them will have whatever is passing for the current state of the art and better design when it comes to patient point of view. Other institutions will have no choice but to go for cheaper options. And of course, there will be fingers, pockets, and the vagaries of salesmanship involved. Business is business, medical or not. What effect does this lack of standardisation have on patient outcomes, on the reputation of institutions? If I was given a choice, I would never choose the particular pump I’m saddled with. At the very least, I’d prefer something which could be carried at or below the waist. Oh yes, I’m sure they all get the job done, and the effect I’m talking about is certainly a small and subtle one, to be sure. Still, I can’t help wondering. Is this lack of a standard also prevalent elsewhere in the world?
ETA: I just didn’t have the energy to do this yesterday, but I talked about it in a correspondence with my friend in colon cancer treatment. Look at the people in that screenshot. Most of them with manic grins and poses, screaming “LOOK AT MY GOOD ATTITUDE! I HAVE POSITIVE!” Fuck that noise. I do not have a positive attitude. I don’t even have a good attitude. I have a shitty, cynical attitude, about most everything, and that certainly includes having cancer. If I lose that, I will be in serious trouble. My colon cancer friend is the same way. So, another little note: don’t go around telling a cancer patient something like “you have a positive attitude, and that’s the most important thing!” No, it’s not the most important thing. It’s not fucking important at all. What is important is whatever attitude your friend or loved one normally has is still intact and firing on all cylinders. If dark, twisted, gallows humour keeps someone going, don’t try to paint it pink with positivity. If razor sharp wit and observations keep someone going, allow that. It’s not up to anyone else to call the shots on what attitude will work best for any given person. As I said before, the person with cancer is still the person you know, they are still the same person they were before diagnosis; cancer is not a call to do a 360 on your personality and attitude.
I was putting off another chronicle for a while, which I’ll get to a bit later, but it turns out today is World Cancer Day. The whole thing is so damn Perky Positive that it exhausts me, but I will say this: If you’re putting off a standard screening, don’t. Grit your teeth, clear your schedule, and get it over with. It may well save your life. The people who love you will appreciate that. Yeah, it can be scary, no one wants bad news. No one wants that news. Nonetheless, Get. It. Done. If you’re stupid like me, and wait until pain shows up, it will be for the worse. If you’re a younger person, and put off something like getting the HPV vaccine, stop that right now, and Get. It. Done. If you’re a parent, and you have not given this gift to your child, Get. It. Done. It’s much better to get that news when you have a good chance of survival. I’ve already known too many people who were dead inside six weeks of diagnosis.
Okay, stories. I was going to put this off until after the next session, but I felt compelled to write today because of the whole world cancer day thing. This involves chemo, having an ostomy, and rivers of shit. If you would rather avoid such shit, now’s the time to stop reading. My next chemo session is the 7th this month, the last two weeks have been a nasty hell spent in a river of shit. I’m exhausted, have next to no motivation to do anything at all, punctuated by bursts of explosive anger. It’s a kind of madness. I’ve had the interesting experience of having constipation and diarrhea at the same time. I don’t recommend it. Chemo turned the shit in my bowels to stone, it felt like I had a belly full of rocks. I waited a couple of days, to see if anything would move, nothing. Yeah, okay, so I take the recommended softener/laxative stuff. That was a fucking mistake. I turned into a skin bag of diarrhea, a spout stuck on ‘pour’. Thing was, this wasn’t coming out the ostomy end, oh no. My belly was still full of rocks, could feel them. This goes on for days. Now I’m taking stuff for diarrhea. Doesn’t work. I’m now on day 8 or 9 of leaking. It’s slowed down some now, and some of the rocks have exited the building, but not through the ostomy end. Feels like all I’ve been doing for over a week is cleaning shit: off myself, off the floor, off the toilet, out of clothes, out of underwear. The only thing happening there is Grimhild burping out farts on a regular basis, and Grimhild has a new trick of rapid shrinking down to flush with my skin, then popping back out again. I’m sure I’ll be having fun with my surgeon again this week. Obviously, stuffing my face like a victim of starvation after chemo is not going to be an option, because I cannot face another two weeks like the ones I’ve been through. Hello mostly liquid diet.
And then there’s the pain. Oh Sweet Crispy Christ, the pain. I have an abnormally high tolerance when it comes to pain, but even I have limits. Why in the fuckety fuck did no one arm me with pain meds before chemo? Why in the fuckety fuck am I going to have to bring this up? Suffering is not good for your nonexistent soul, it isn’t good at all. Out of my current doctors, only the radiation doc was familiar with the direct and referred pain caused by a colorectal tumour, and I’m wondering why. The pain has prevented me from sleeping, it’s woken me up from sleep. It overrides everything and leaves me wanting nothing more than to be unconscious. A low down (no pun intended, but…) colorectal tumour makes your tailbone a center of pain, it spreads out over and through the ilium, the lower spine, and puts amazing, blinding pressure on the sciatic nerve. It’s so gosh darn fun to get up and think you’re going to walk, and have a lightning strike of pain take your leg out from under you. That kind of pain momentarily shocks you out from under the dismal symphony of pain which has already become oppressively routine.
Sitting at my desk, staring off into middle distance, I become aware that I’m nodding along to the rhythm beat of pain in my lower spine rather than the music playing. Time for inadequate meds again. It’s a piss always having to be medicated, too. Well fuck it, I have animals who would like to be fed, so I’ll go do that. For the record, rats totally win on the “oh gods, we are going to die right this second, pitifully, in your arms, if we aren’t fed immediately!” There’s nothing like walking in and seeing a group of boys standing up and reaching their little hands out like a chorus of Tiny Tims.
Why in the fuckety fuck did no one arm me with pain meds before chemo?
I believe that there is a certain christian/religious bias toward suffering, which manifests in American tendencies to not relieve pain when it can be relieved. If we were a rational society, we’d not be asking “how do we regulate opiates?” we’d be asking “how to we produce amazing painkillers that anyone can have, recreationally or otherwise, that have no negative side effects?” There’s this aesthetic of suffering built into religion that, I believe, permeates the whole ugly landscape.
The only evidence I can offer to support that belief is that suppressing pain would benefit capitalists; therefore it should be a sacrament. What boss wouldn’t love their employees to be able to spend a weekend in a happy stupor so they can come in bright and perky (on other drugs) to work on monday? In that context, I’d expect capitalists to be trying to figure out how to put the aged and dying to work driving ubers, or… oh. right. They are.
Oh, I don’t need evidence of that belief, it’s blindingly obvious to every single pain patient.
Caine@#2:
Oh, I don’t need evidence of that belief, it’s blindingly obvious to every single pain patient.
Fucking pain-fetishists. They’re sadists but they’re not self-actualized enough. If they were, they’d at least be able to enjoy gloating -- that’s much more fun than feeling sanctimonious.
Good ratty Tiny Tims you go on distracting Caine.
Pain serves a function to warn of injury, but it doesn’t do anything useful when you know what is causing it, and the body’s reactions to it, like tensing round the pain, tend to exacerbate the pain with no gain. It’s fucking useless when it’s referred pain like the sciatica. Such well designed bodies we have /sarc. Sorry you are getting the sharp jabs as well as the constant back ground pain, neither is good, but pain that makes it impossible to move or speak is the worst.
Marcus:
Oh, some of them do. There are always some of them in the world of pain medicine. Fortunately, you don’t smack into them often, but the sanctimony is everywhere, and it’s bad enough.
Jazzlet:
Fuck yes.
Lack of standardization is always a big problem. The problem in USA seems to me a combination of authortitative state and libertarian one, where combined are the worst elements of both. Pain killers -- authoritarianism that harms patients. Chemo pumps -- pseudo free market build on making a profit of human suffering.
Drugs completely without side effects, especially drugs that affect the nervous system, are unfortunately impossible to achieve, but a reasonable compromise is probably somewhere in the aether to be found. And before those drugs are discovered, a resonable (emphassis reasonable) regulations are in order. Universal healthcare is for example a regulation. And it would undoubtedly lead to reduction of illicit drug use, improvement in patient care, reducing costs etc. It has been proven and demonstrated multiple times in recent history and around the globe, but American governing elite refuses to see the evidence for this, just as they do with guns.
Caine, I cannot imagine what you are going through. I hope the pain becomes bearable and eventually goes away, with, preferably, apppropriate medication in the meantime. Fingers crossed.
*hugs*
I’m sorry you are going through this. Hopefully funny ratties bring some smiles!
@7 -- that’s an interesting observation. Our health care system isn’t even a system -- it’s such a disconnected patchwork mess. Too often scary for patients w/ multiple docs or specialists as one can’t be sure if all the docs are on ‘the same page’ and know what is going on w/ one patient due to that.
We do indeed have the worst combo.
I’m hoping things will eventually get better for you. Please keep on writing on these things as long as it helps you get by.
While I think an universal health care could be an improvement, there can be local differences. Here, municipalities* and organizations in which neighbouring municipalities co-operate are responsible for the universal health care and each municipality or organization does their own purchases/organizes competitive bidding processes.
I’m not sure, to what extent do the national standards and recommendations influence these things. Sometimes you do have to buy your own things to get what you need now, like my blind friend had to buy a talking blood sugar meter and test strips for it when he became a diabetic. He later got a similar meter for free and now gets the strips he needs regularly. I admit, I don’t have an extensive experience about these things.
__
* = This isn’t insurance mathematically ideal, as a small municipality can get into deep financial trouble if someone gets some rare but expensive to treat condition.
That pain thing… that just really sucks. Very sorry about it. I do hope someone gets a clue and you can get the pain under control.
I had a friend with chronic pain (hers was her back) and she explained to me that people who abuse pain killers do it to move away from society, whereas people who are in pain use pain killers to move *towards* society, they use them to normalize themselves so that they can live a normal life. When she said it I thought, man, that does not seem like such a big thing to ask for. So WTF? Why not try and help chronic pain people? SO frustrating…
Too many doctors just don’t understand pain control. Even the ones that do are reluctant to order properly because of concerns re addiction, which is nonsense because when the pain leaves so does the need for pain control in the vast majority of patients. If the pain persists so should the pain control. If you have a nurse case manager talk to them. Oncology nurses will likely have more time to listen and teach than the doctors do and the good ones will advocate on your behalf. I would also recommend seeing a nutritionist if one is available.
Caine, I keep saying that I’m sorry and I hope things improve for you. That’s all I know to say, but I really mean it.
Thank you all very much.
Kestrel:
That’s true. I don’t know any group of people less interested in getting ‘high’ than pain patients. We just want to be pain free. I can’t imagine anyone getting ‘high’ on my meds, or even the stronger stuff. All that matters to me is the moment ‘pain is less or gone’ registers. Then I can get some shit done. On those rare occasions I’ve actually hit ‘completely pain free’, Rick is always overwhelmed by the change. He tells me “you’re energetic, eating, talking!” That’s a pretty low bar for every day goals, but trying to get adequate pain meds is a constant fight. It’s no surprise at all that people are always going for an end run around the system, because it sucks.
Voyager:
Yes, true. My oncology nurse is fantastic, and I couldn’t say enough nice stuff about her. I don’t get to talk with her much though. I have what is called a ‘navigation’ nurse, and she is kind and enthusiastic, but…she’s Ms. Baking Soda for mouth sores. That’s another thing I have to write about, I keep forgetting. Well, next time.
Sorry your navigation nurse is underwhelming.
The whole idea of getting high on pain killers makes me give a hollow laugh when anyone raises it. I have never got anywhere near being high, just as you say had those wonderful pain-free times. As far as I understand it people with chronic pain are extremely unlikely to become addicted to pain killers because we don’t get high, the drug is all used up dealing with the pain. Yeah I suppose you could say I’m addicted to being pain free, but that’s nothing like getting high, and anyway most people are.
Jazzlet:
Exactly. We still get to pay the price for the intense fear of potential addiction, though. There have been times when I’ve had to go two weeks without my scrip meds; the pain is bad of course, but I have never had one single “withdrawal” symptom. I wouldn’t have the slightest idea of what one looked like. I have exactly one side effect from the hydrocodone, and that’s only if I take more than one, which I usually do, against instructions, because one doesn’t do jack fucking shit. Anyway, I get chatty for about an hour. That’s it.
If I was looking to get high, it wouldn’t be with the stuff I’m given, anyway. There’s much better product out there, and downers were never my thing. I much prefer speedy stuff, which is probably why I get so happy energetic when I hit pain free (which does not happen often) -- it doesn’t feel normal, that, it feels downright abnormal.
@1 Marcus, sorry to jump in so late to the thread. I was dealing with my own pain this weekend. Whether you believe it or not, we are taught to control pain immediately, from the beginning of any illness A high tolerance to opiates makes that more challenging, but not impossible. And you are correct, many doctors don’t understand pain control. I was lucky enough to do some of my training under Dr. Russell K. Portenoy, one of the parents of modern pain medicine. There was a massive epidemic of untreated pain in this country in the 1980s. And the people who were most ill-served were at risk populations: women, minorities, children, LGBTQ, the elderly, poor, the mentally ill. Dr Portenoy wrote the seminal paper that promoted the usefulness of opiates for chronic pain. Not everyone gets to train with a thought leader. And not every doctor is receptive. I sought out my fellowship program because of my interest in palliative care, but some doctors don’t give a damn. They bring their preconceived notions of right and wrong and health and pain with them to medical school and never bother to learn anything else. No one should be in pain. It’s a doctor’s responsibility to see to that. We may not always succeed, but we should always try.
Caine, “Oh Sweet Crispy Christ” made me laugh out loud. I frequently reference a certain Deep Fried, Sugar Coated Baby Jesus on a Stick (purchased at the County Fair) in moments of frustration. It is sweet delicious blasphemy.
Raucous Indignation@#17:
Thanks for the info.
I’m part of a “Hopkins Family” (Dr Heyssel was my next door neighbor when I was kid, ffs! And the head of the teaching faculty of diagnostics lived on the other side of us.) and I worked at JHH as a systems admin in 1987-9 -- part of what I loved about working there was seeing how the technology went from research to prototype to fielded to used worldwide -- I was a test volunteer for V1.0 PET scanner and worked with Eliot Fishman on 3D rendering the first data-sets for reduced intrusiveness surgery. It’s fascinating to see how long it takes for word of some things to percolate fully out.
One of the things I worked on was a thing called the “clinical workstation system” -- basically, a medical google thing that could be near surgical theaters, etc. And we did a lot of human factors research and discovered that 9 out of 10 times, if a doctor didn’t know something, they’d call their golf buddy or their college buddy. Even if they were in a different field. That was interesting. But I worked there long enough to see it change to that some doctors would call their secretary and have them look something up. One doctor declared, “I will never touch a keyboard.” It’s changing.
Thing is, more and more pain patients are shunted to pain clinics, rather than dealing with individual doctors, who are generally quite responsive to pain issues. Pain clinics are often allied with the feds, and part of the “drug watch” system. Mine is, so in order to receive pain meds, I’m subjected to drug testing, not just for illicit drug use, but whether or not my scrip drug usage matches what they think it should be. If it’s determined to be “too low”, you can be turned over to the DEA for possible dealing. People also act like 10/325 hydrocodone is this super powerful drug with addiction potential, instead of a barely jumped up acetaminophen.
This fucking nonsense can be bypassed by going to an individual doctor, but ever since the feds changed the schedule on all opiates, a lot of doctors won’t prescribe, because of the hassle of not being able to do refills, so people are referred to pain clinics. It’s a right pain in the ass for me, too, having to count every 21 days, and putting in a request to the pain clinic via my pharmacy, then picking up the following week.
Ooof that all sounds brutal. I’m not sure if its something possible for you to do, but once I got out of the hospital after my surgery my GP got me set up with a pain management doctor to handle my chronic pain meds. My pain specialist has been really helpful in finding a regimen that works well for me. He was responsive and helpful when I needed to increase my script for traveling and the inevitable bad nights. Of course I’m not back to what use to be normal but I think normal is something that is going to be different from now one. I’m also not trying to go with too high a dose as I don’t want my tolerance to climb to fast. One other thing that could be helpful is that, when I was meeting with the doctors before I had surgery, they prescribed me a steroid that caused the inflammation around my tumor to go down. Since the tumor was pressing on some fairly important nerves this lead to significant symptom relief. I’m not sure if steroids are things you’re already prescribed or if they are contraindicated but they could help with the tumor pressing on nerves.
I will say that my ostomy got better the longer I had it. It was weird when I had it put in, but I had nurses at the hospital to help me get through the early bit. I’m not sure if yours is going to be permanent or if you can have it reversed later but after a year it looks a lot less brutal and its not to bad to manage.
square101:
I will definitely check that out, thank you! I already get steroidal spinal injections, and the same injections for shoulders and upper back. There shouldn’t be any problem adding another steroid in. The nerve pressure is just brutal, well, I don’t need to tell you. I already get enough of that when my bad discs get inflamed and swollen.
Oh, the ostomy. Well, hopefully it’s temporary, but I’ll still be living with it for a considerable amount of time, as of right now, surgery is slated to be the very last thing on the treatment list. That’s the one thing I’ve had the least trouble with. I was home with mine four days after surgery, and I would have appreciated more information, but there are things no one can tell you unless they’ve been through an ostomy themselves.
As far as basic information, I wish to hell someone had warned me off those damn barrier wipes. I didn’t have them right away, and should have realized I didn’t need them, but they are sold as a skin protectant, which is very misleading. I did not have any problems with my bags adhering, and I’m quite thin, so no problems with skin folds or anything like that. Using one of those damn wipes had the bag near to superglued onto my skin, and I actually lost a fair amount of skin in the removal. It took ages to get the plasticization from that off my skin.
@20
Sorry, I didn’t see your post before I wrote mine. That is completely ridiculous. I’ve heard about people being tested to make sure they were using their meds before but I thought that there would have to be like a reason to suspect that they were dealing. Testing cancer patients is just cruel. I also hate the very specific prescription that they have for opiates and if you can’t get it refilled right away you’re just shit out of luck. I understand that people who have problems with addiction can use method they can to try and get drugs and that can make health care professionals not great at trusting patients. But i feel like if you actually have a verifiable diagnosis maybe people could chill their shit and try to help these people feel some semblance of normalcy.
square101:
Exactly. The feds don’t care to even try to accommodate pain patients though, it’s a “stomp on everyone” law. To clarify, my pain clinic stuff is for my spinal pain, it has nothing to do with the cancer. I don’t go back to pain clinic until the 14th this month, and my appts are every 3 months, so the last time I was in, I had not been diagnosed yet. I have no idea if they’ll suspend the drug testing for the duration of treatment, but I doubt it.
I’ll be able to talk with someone about pain meds for the cancer pain this Wednesday, when I’m back in for more labs and another chemo session. I know if/when the nausea sets in, I won’t hesitate to use weed, but the medical weed program only went into effect here this month, and it’s not even set up yet, so whether or not I can do that legally, I don’t know. If I can’t do it legally, then I’ll have to forgo the meds for my spinal pain to get out of the drug testing.
@22
I’m not sure where you get your supplies but I use an online ordering place and once of the things they offer is Brava adhesive removal spray. My stomach is pretty hairy and unless I was shaving basically every time I changed flanges I was pulling out a good amount of hair each time. With the spray it peals off super easy and I’ve had no problems with it afterward and one of the bottles lasts around 2 months changing twice a week. I don’t know what your exact situation is but they even sell it on amazon for about $15.
@17
I know exactly what you mean about the tollerance. I know with some specific opiates like codine the bodily metabolism plays a heavy role in its activity since it has to be converted to morphine by the liver. I’m not sure how it applies to other opiates but I feel like I must be a fast metabolizer since they all seem as potent as expected but lasted ~1/2 to 2/3 the amount of time expected. This was the worst problem in the hospital. Due to the med vending machine the nurses had to get the opiates out of they couldn’t give me 10 mg of oxy every 2 hours but they could give me 20 mg every 3 hours. This all meant that I had to take big doses so that I wasn’t stuck with an hour and a half of pain between doses. I think it is lucky that i’m not a person who find opiates very uncomfortable or too comfortable. I ended up with a pretty high tolerance to the opiates when I left the hospital since I spent the first two weeks waffling between being in pain and basically sleeping away opium dreams. It could have been a lot worse but it was really aggravating that I couldn’t have the meds spaced out it the manner that I wanted. I mean I wasn’t even asking for more meds i was actually asking to have less meds per day just on a more consistent level.
Its been interesting working with my pain doctor since I’ve always been interested in drugs both medicinal and recreational. One of the great things he worked with me on was switching part of my dose to methadone instead of oxy which helped create a more stable baseline that wasn’t perfect but at least made the ups and downs more stable.
Caine, it is no longer appropriate for your pain to be treated out of a pain clinic. You describe malignancy related pain far in excess of your chronic back pain; you should transition to your cancer center’s pain medicine and palliative care team. You shouldn’t ever have pain like that. I admitted a patient to our regional medical center last week just so I could get control of her pain. 10 over 10 pain means you need to be moved up the “cancer pain ladder.” Did you let your care team know? Maybe they can schedule a pain med palliative care appointment for you when you’re in Bismark?
And yes, you are correct; hydrocodone/APAP ain’t nothing more than jumped up acetaminophen.
@24
So the cancer diagnosis may actually help you get pain meds now. Before I got set up with my current doctors I went to a nurse practitioner after I had the diagnosis because the pain had finally gotten significant enough to need meds better than over the counter ones. He flat out told me that that the only reason I was getting pain meds from him was cause I had cancer. He said that they basically see the risks of prescribing opiates worth it when you cross the line from some other chronic pain conditions to having cancer. Of course this may not be the way for everyone but I certainly hope you can get someone to prescribe the meds you need.
If you can use it without having to worry about drug tests and it is your style then yeah I would recommend cannabis. I smoked recreationally a few times a week since undergrad especially since my state legalized while I was in grad school. Ever since getting out of the hospital I’ve been smoking fairly regularly every night. It lets me use the pharmaceutical meds for while I’m at work and need relief without significant intoxication and then when staying sober is not important I can smoke. Its odd sometimes talking about it online because I feel like I’m actually a more frequent smoker than many people online who scream about how cancer is a miracle drug but I’m fairly conservative in my recommendations. The opiates are better pain meds but the cannabis works ok if I can just sit around the couch. Similarly I’ve heard the prescription nausea meds work better than cannabis but the weed can kind of calm the nausea and can make it easier to ignore it. If they just started up the medical program in your state it may be difficult to actually find weed unless you already have a pre-medical hookup but it should be find-able.
@25 Square101, codeine is worse than garbage. It must be metabolized into an active form, but it comes at the expense of many and varied adverse effects. Many more side effects than a pure mu-agonist like morphine or hydromorphone or oxycodone. So that’s great. Everyone gets shitty side effects and few get adequate pain relief. I haven’t prescribed codeine, not even as a cough suppressant, in maybe a decade? Maybe 15 years?
Those vending machines are to keep close control of all the controlled substances. But they only dispense what the the doctors have ordered. If your doctor orders 20 mg every three hours, that’s all that can be dispensed. No more, no less. Proper pain orders would include a long acting opiate for long acting control and then two separate orders for breakthrough pain, one for pain level 4-7 and a higher one for pain level 8-10. Most opiates are effective for 3-4 hours, so at least your doctor got that correct. Some doctors will order pain meds every 6 or 8 hours apart. Which is plainly cruel when your average duration of effect is only half that long.
Raucous Indignation:
Not yet, I’ll be doing that on Wednesday morning.
@19 Marcus, dude, I kinda knew you were old but crap almighty! Things changed decades ago; this “new thing” called evidence-based medicine is really old! You really worked with doctors that couldn’t use a computer!? We used a computer every morning on AM rounds when I was an intern and I’m old as dirt!
Caine, please reach out to them. They sound like a good team. They will help you.
Raucous Indignation:
I wish you could come down like thunder on the pain management at my pain clinic. They expect me to take 1 jumped up acetaminophen every 6 hours, like that would be all great and take care of the pain. Same with the 50mg tramadol. I try to be honest with them, but it’s hard. I take more than 2 jumped up acetaminophens a day, to say the least. When the pain is mild, I don’t usually bother at all; when it’s bad, I take what I need to for actual pain relief. They don’t last long with me; max, I get 3.5 hours.
I’ve tried taking one hydrocodone. Absolutely nothing. Zip, zero. The few times I have ventured to mention this, it’s met with incredulity. It has nothing to do with tolerance, either, it’s been that way from the start. The only reason I take the tramadol is because it seems to potentiate the hydrocodone where I’m concerned.
Raucous Indignation:
My late neurologist did not like them, at least not the hospital computers.
@28 Raucous Indignation
Yeah we talked to the nurses and the doctors about it. The docs at the hospital were great about making sure my pain was controlled, especially when I made myself a new 10 on the pain schedule the first time I tried to get up. The main issue with whatever inventory control system they used is that you could only dispense 20 mg every 3 hours. They said that if they had tried to give me 10 every 2 hours when they went to open it for the 2nd 10 mg dose it would reset the clock to 3 hours instead of 2 so they just had to give me enough so that it wouldn’t wear off. They had me on a 30 mg of extended release oxycodone every 8 hours, however since it was taking ~15 mg of immediate release every 3 hours to control the pain i don’t think the oxycontin really offered much benefit. Since my pain is much lower now the methadone works great as a long acting baseline medication. I was also started on both lyrica and gabapentin for nerve pain too. It was an interesting 7 weeks including physical rehab hospital.
@Caine
One thing I forgot to mention is that the best thing that has worked for me constipation wise without causing serious diarrhea was miralax. Taking it every day it didn’t speed up my bowel movements but it has kept the opiates from causing anything to get hard. Once I started taking it everyday I didn’t have any problems even if I don’t have daily bowel movements unlike a couple times before surgery when the pain meds gave me a decent amount of constipation. My constipation was caused by the opiates not chemo so that could make your situation different.
And one hydrocodone every 6 hours is what they gave me when I got my wisdom teeth out. It was nice for wisdom teeth, but is no where enough for what you have.
@34 Square 101, hrrmm, that’s odd. Maybe the institution has some sort of maximum built into their system, which is nuts because the great thing about opiates is that they don’t have a maximum ceiling.
Caine, please tell me you’re not being given both hydrocodone AND tramadol? Rather than potentiate hydrocodone, tramadol can usually be counted on to act as a partial opiate antagonist. But it works the opposite for you? Hrrmm … I need to think about that.
I probably will do a literature search ON MY COMPUTER! Sorry about the shouting; that was for Marcus.
I personally found senna-s at bedtime the most effective thing for opiate-induced constipation.
Caine, it really sounds as if your pain clinic is managing your medication consumption and pill count rather than your pain. And how exactly do they track your consumption with urine tests? I wasn’t aware that was possible.
I take senna at bedtime and Laxido during the day whenever I can fit it in round taking pills. Because Laxido works by keeing water in the gut (and so keeping the shit soft) it can also keep other things in the gut like the ingredients of pills, so you aren’t suposed to take pills an hour before or an hour after taking the Laxido. Can be difficult what with the every eight-hours-pills and the take-as-needed pills, sometimes I just have to wait to take the next lot of take-as-needed pills. Of course if I could manage to have a nice regular lifestyle it would be easier, but that seems beyond my reach at the moment.
Caine I really hope your cancer team can help, you shouldn’t have to be in pain or to have to plead for pain relief, it’s so fucking humiliating.
Raucous Indignation:
Yes, my scrips are for hydrocodone and tramadol, in the dosages mentioned above. Tramadol on its own doesn’t do one single thing for me. And yes, for some reason, the tramadol taken with the hydrocodone works well with me. I have no idea why, but I’m not a terribly reliable person when it comes to med reactions. Initially, my neurologist switched me over to tramadol when the schedule changed, because he didn’t want to deal with the no refills business. He told me at that time if I wanted to continue with the hydrocodone, I had to do it through the pain clinic. The tramadol wasn’t working on its own, so I went to pain clinic. The combination works better for me than either on its own.
One thing I don’t get is opiate-based constipation, they just don’t affect me that way. Of course, I’m getting such a tiny dose, maybe it isn’t enough for that. But, I had plenty in hospital, and no constipation problems. As for senna, doesn’t do one little thing where I’m concerned.
I’m not privy as to the details of the piss tests, but you are always asked if you have taken meds that day, and if you haven’t, when your last dose was taken. You also have to say if you’re doing something like eating foodstuffs with poppy seeds, and so on. I’m not subjected on every visit; I’d assume if a pain management person was suspicious, they would up the tests. As far as tracking, I would assume what they are looking at is a pattern, not an individual test. If you keep coming up as under what your level should be, there’s a suspicion as to why. I really have no idea at all if this sort of thing is the same from clinic to clinic, or from state to state. I also have no experience with a clinic which is not partnered with the feds in the whole drug watch business.
square101:
Pardon me, but OHGODSNONEVERAGAIN. *cough* It was bloody miralax which was recommended to me by the navigation nurse, and that’s what I took for the initial chemo induced constipation, and it’s that which turned me into a nonstop diarrhea faucet. You could not pay me enough to ever get near that stuff again. I don’t get opiate induced constipation.
I am envious, Caine. One Percocet and I won’t poop for a couple of days.
I think random urine testing is worse than useless. The number of false positive and negatives makes serial testing uninterpretable. Maybe the testing is better than it used to be, but I doubt it. Lab personnel are still as variably and unpredictably fallible as they’ve always been. Most lab error is because of operator error, not flaws in the method.
The entirety of the delivery of health-care in the USofA makes me sad.
The technology is probably the best on earth but the delivery is managed by baboons.
Baboons who have an agenda. And a grudge against the neighbo
uring troop.Well shit, pun not intended, miralax was the only laxative that actually did something, senokot never did a thing, with out giving me the shits, which ducolax always did. I’m lucky that I think my body has gotten use to the dosage that I’m on and things have settled out. I will say I never noticed any opiate constipation until I was taking 15-20 mg of oxycodone a day for about a week or so.
It’s great that you don’t get opiate induced constipation. Before all of the meds I take were sorted out I ended up with constipation so bad I thought I’d split something in my head getting the bastard out, worse headache ever, worse than migraine even, though no stabbing through the eye thing (my migraines feel like I’m being continually stabbed through my right eye with associated visuals of flashing with the stabs).
The whole pain clinic set up seems nuts, completely barking.
Jazzlet:
The opposite nightmare to mine. Yikes.
Yeah, seems that way to me, too. I can’t just go and get my injections and put my med requests in; I have to meet with pain management every time, for no real reason. Just goes over the meds, basically. It’s a system designed to always let you know you have zero power.
Caine, what you said makes me so sad. “It’s a system designed to always let you know you have zero power.” That’s not how any medicine should be practiced. I am the patient’s consultant and advocate. I quite literally work for them. The practitioner is supposed to be the caregiver, you know? As in, giving care to the patient. The idea that people in pain should be stigmatized and degraded is medieval. That has no place in modern medicine. I hope you can transition your pain management to your cancer team.
Good luck tomorrow. Hugs.
Well, it’s not like being put on the rack or anything, but yeah, you always know that you must be compliant, or else. Some of my pain clinic people read Affinity, and all this probably won’t go over well; but they’re stuck in the same system, and they have to be compliant too.
Thank you. :)
jazzlet@#48:
It’s great that you don’t get opiate induced constipation. Before all of the meds I take were sorted out I ended up with constipation so bad I thought I’d split something in my head getting the bastard out, worse headache ever, worse than migraine even, though no stabbing through the eye thing (my migraines feel like I’m being continually stabbed through my right eye with associated visuals of flashing with the stabs).
When I had my kidney stone I had some similar issues. Severely. It was exceedingly unpleasant. If you can start taking a glass of metamucil or miralax every morning as soon as you go on the opiates, it prevents the problem from occurring.
Dehydration is another problem, which also magnifies the constipation. My theory is that the nerves that carry “I am thirsty” and “I am hungry” are probably evolved from pain signals, so the painkillers suppress those signals, too. If you put yourself on a scheduled “drink this much water” and “take this much metamucil” you’ll be OK.
…. now that it’s thoroughly too late to help you, he says.
Well shit, pun not intended, miralax was the only laxative that actually did something, senokot never did a thing, with out giving me the shits, which ducolax always did
By the way -- one thing that I would say is contra-indicated is ex-lax.
What ex-lax does is tells your intestines to start moving the train along. “Ding! Ding!” the train tries to leave the station. But it doesn’t fit in the tunnel. Then, since the train has been TOLD to get moving, it starts relentlessly trying to shove its way into the tunnel, anyhow. “Ding! Ding!”
I had severe constipation and managed to relieve it by irrigating myself using a syringe and some mineral oil and water and letting it sit for a few hours. But, “Ding! Ding!” the fucking ex-lax had told the train driver to keep trying to fit through the tunnel every couple minutes. Violently. It was horrible.
In retrospect, I am a bit annoyed that they don’t tell you about these things when they give you the opiates, or that they don’t give you the opiates along with some miralax. They also tell you “make sure you eat” which, IMO, is too casual. They should be telling patients, “no, really, you need to schedule a time each morning at which you eat miralax or metamucil and ${calories} or you will fall off a calorie-cliff and collapse and die. The last late-stage cancer patient I watched die -- that was what happened to him: it hurt to eat and make the train run on time, and the opiates obviated that pain, so he stopped eating and everything else stopped, too.
Miralax, btw, appears to be a fine powder of those hydrophilic water beads that I enjoy playing with -- the squishy, slipperly, bouncy stuff that sucks up water and holds it? Yep. Maybe someone’s kids ate a bunch of the beads and they went, “hmmmm…”
@50 Marcus, Marcus, Marcus … I don’t know how to break this to you, but bulk agents are relatively contraindicated for OIC [opioid induced constipation]. Opiates slow transit thru the colon allowing the colon to extract more water than usual from the stool thus making it harder and larger. Adding fiber or bulk just makes that process worse. You could end up with massive concreted stools impacted in the rectum if things go wrong. (I have been there; I have relieved such obstructions; it is not good.) We recommend agents that increase the water content of the stool and/or promote more rapid transit through the colon.
You are correct about Ex-Lax. I can’t think of a legitimate medical indication for Ex-Lax.
Miralax is just a long chain polyethylene glycol with neutral tonicity salts so your electrolytes don’t go all wonky. Shorter chain PEG are used in more or less everything. I can almost guarantee your shampoo contains PEG. Probably your toothpaste too. It gives your colon a salty shampoo!
Raucous Indignation@#52:
You could end up with massive concreted stools impacted in the rectum if things go wrong. (I have been there; I have relieved such obstructions; it is not good.)
Yeah, me too. Let me just put it this way: “that was some scary shit.”
I managed to deal with it, but it was not something I ever want to repeat.
Good to know stuff like Metamucil is contraindicated. I wish they’d have told me any of that stuff. I don’t think it’s good patient care to go, “well, here’s 2 oxycodone” (it’s monday) “you ought to be able to see a urologist by friday” (that’s 4 days. 2 oxycodone? thank goodness I have an illicit stash or I’d lose my mind from the pain)
I didn’t realize the opioids slow the train down. Now it all makes more sense.
Many years ago my dog Miles had a problem when he swallowed an entire rabbit. The skull wouldn’t fit out the back end of the dog. So an unfortunate vet tech had to spend a while irrigating him and walking him about until he finally exploded. I basically did that, all alone here. I certainly had a lot more sympathy for my dog (not that I lacked sympathy for the big sweetie to begin with!)
Raucous Indignation:
Given that miralax turned me into a non-stop diarrhea machine, what, exactly, do I do for the chemo induced constipation, which is just like the opiate-induced -- concrete shit?
I’m not sure, Caine; everyone is a little bit different. You had mucositis with your first cycle which is usually accompanied by diarrhea, not constipation. I think start slow with something like Colace and then add Milk Of Mag and/or senna. There is a big variation in potency of the various senna preparations, but you can always take three or four tabs if one or two doesn’t do anything. Of course you could stick with the Miralax but only take a half or third dose of a dose? To say nothing of Mag Citrate and lactulose and …
Lots of options. Be gentle, go slow.
And then nuke your colon from orbit if necessary. It’s the only way to be sure sometimes.
Ah, but I do have constipation! The cement shit is still working its way out my ostomy end, while diarrhea pours out my arse end. And, I have more chemo tomorrow morning. And I know it’s bad, but I’ve already stopped eating, outside of some ice cream now and then, because this is all driving me crazy. There was no diarrhea until I took the miralax. Just constipation.
Oh, and chemo gives me nosebleeds, too. I’ll keep the nuke in reserve.
Yeah, the fact that you have two different parts of your colon behaving in opposed manners does sort of complicate this. And I don’t really know the full extent of your tumor burden or actual toxicities, soooo I’m all kinds of swinging here. I again think you should start with Colace and maybe some MOM?
Yeah, nosebleeds too? I’m having a little trouble keeping up with your symptoms. I think I’m gonna have to bill you out as a 99214 today.
Raucous Indignation:
I’ll give it a shot, it can’t be worse than what I’ve been through. The next two weeks ought to be a blast. I have a feeling I’m going to end up being the exasperating patient from hell. And you probably should bill me, for all the free medical I’m getting from you!
Eh, nosebleeds. I was subject to spontaneous ones when I was young; they’d hit for no reason, and take forevah to stop. I still remember being kicked out of kindergarten class because of one. The teacher was freaking out over all the blood, and didn’t want the other sprogs to be scared, so she gave me another towel, and shoved me out the door, to stand around by myself until the bleeding stopped.
Highly compassionate and ethical teaching, so lucky younger you was, so lucky …
Can I say how much I appreciate a place to talk about shit?
On a more serious note, you’d think that the most sensible thing to stop people from abusing pain killers would be to remove their pain, but that would mean caring about people.
Raucous Indignation:
Oh, about 20, 30 minutes later, a nun came walking up, wanting to know why a bloody 5 year old was hanging out right by the street. I mumbled “nosebleed”, was hustled to the nurse, and I do believe the nun went to have a chat with the teacher.
Giliell:
Thank you. Me too. :D
Well, yeah. It’s all pretty simple, really, but things are so fucked up here, I don’t know, it would take 3 or 4 revolutions to start fixing it. One major problem is that people try to ignore minor pain, and it’s hard to get anyone to take that seriously, but it adds up.
I mentioned earlier that part of my training was under Dr Russell Portenoy. His remarkable contribution to pain medicine was this. There is no objective measure of the patient’s pain. Nothing reliably tells you how much pain a patient is suffering.He cannot rely on vital signs body position or facial affect. Dr. Portnoy’s great breakthrough was to ask the patient how much pain they’re in and then believe what the patient tells you. Believing your patients was the radical breakthrough in the way we treated people who complained of pain. It is so fucked up that we ever practiced medicine any other way.
Marcus @#50
Thanks for the thought. I’m reasonably sorted now with a stool softener like RI was describing The main proble is you are not supposed to take it within an hour of taking pills or take pills an hour after you have taken the softener which sometimes means I forget to take it -- some of the pills I’m on can make me a bit fuzzy which doesn’t help.
I too appreciate having somewhere to talk about shit! the only person I know who reallyunderstands what I am talking about about shit is one of my brothers who has colitis, therefore also has shit stories and is happy to have the odd exchange on ‘shit that has happened with our shit’.
I hope the appointments tomorrow get you some help Caine, both with the pain and with the odd things your guts are doing.
Thinking of you today, Caine
I have no directly useful contribution here, just wanted to say I am learning lots of interesting and useful things from this conversation, making it both 1) excellent and 2) deeply unlike the comment section on every other part of the Internet.
Abbeycadabra:
There’s absolutely no need to feel like you should make a ‘useful’ contribution; I find everyone’s comments to be useful, and if people learn stuff, that’s all the better! I know I’ve been learning a great deal from people in these threads, so it’s definitely helpful to me!
Yeah, these threads are unique, and I hafta say, I love them.