Via Kevin Drum I came across this graphic that shows that health care costs in the US are much higher than those in other developed countries. This should, of course, come as no surprise to anyone.
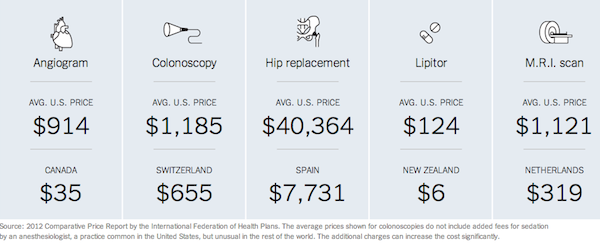
But why is this the case? Many of the easy answers don’t quite cover it. This article by Elisabeth Rosenthal from which the graphic is taken looks at possible explanations.
Whether directly from their wallets or through insurance policies, Americans pay more for almost every interaction with the medical system. They are typically prescribed more expensive procedures and tests than people in other countries, no matter if those nations operate a private or national health system. A list of drug, scan and procedure prices compiled by the International Federation of Health Plans, a global network of health insurers, found that the United States came out the most costly in all 21 categories — and often by a huge margin.
Rosenthal looks at the case of colonoscopies., which provides an excellent case study of how in it seems like we in the US tend to go with the most expensive option for treatment.
Largely an office procedure when widespread screening was first recommended, colonoscopies have moved into surgery centers — which were created as a step down from costly hospital care but are now often a lucrative step up from doctors’ examining rooms — where they are billed like a quasi operation. They are often prescribed and performed more frequently than medical guidelines recommend.
The high price paid for colonoscopies mostly results not from top-notch patient care, according to interviews with health care experts and economists, but from business plans seeking to maximize revenue; haggling between hospitals and insurers that have no relation to the actual costs of performing the procedure; and lobbying, marketing and turf battles among specialists that increase patient fees.
While several cheaper and less invasive tests to screen for colon cancer are recommended as equally effective by the federal government’s expert panel on preventive care — and are commonly used in other countries — colonoscopy has become the go-to procedure in the United States. “We’ve defaulted to by far the most expensive option, without much if any data to support it,” said Dr. H. Gilbert Welch, a professor of medicine at the Dartmouth Institute for Health Policy and Clinical Practice.
All those other countries that have cheaper health care costs have some form of universal, government-run, single payer health systems. It is crazy that the US is the one holdout on this issue among all the developed countries and many of the developing countries.
As a European, the US healthcare system is simply baffling, I don’t understand how anything so spectacularly expensive and inefficient can be defended by so many people.
The company I work for recently went bankrupt, so a lot of people were suddenly finding themselves scrambling to find their own private insurance schemes.
Why?
Why, in the name of christ, do those two things have anything to do with one another? And what happens if you become too ill to work? You lose your job and consequently lose your healthcare, it’s madness!
I can understand companies providing a higher level of healthcare as a perk, but basic healthcare should be provided as a fundamental civil right.
I don’t have an answer and I’m not sure that there is “an” answer, but a couple of thoughts…
1. The prices listed above are wrong. They are what the hospital or practice charges, but not what they get. For example, Medicare routinely pays 40% of charges, when they don’t deduct further for minor errors in paperwork. So the $1185 colonoscopy is really priced for medicare at $474. Medicare is one of the better payors.
2. The hospital I work at employs three people, full time, to do nothing but go through charts and make sure that every note is signed, dated, and timed. Not for any patient safety issue, but simply so that the insurance companies won’t deduct anything for failure to complete the note. So there’s about $200K/year of costs for virtually nothing.
3. Insurance companies pay people specifically to make sure that claims are denied. This results in a lot of wasted effort and resources as the hospital struggles to get the money it is owed (often by inflating the costs and settling for a percentage) and the insurance company struggles to avoid paying.
TL;DR version: Single payor: faster, better, cheaper.
Hi,
Hopefully you read this with the recent Time article by Steven Brill in mind as well.
(pdf here -- http://livingwithmcl.com/BitterPill.pdf )
Although very complicated, it certainly boils down to being a seller’s market, with sellers controlling the profits and buyers largely without choice or knowledge.
We speak of “health care reform”, but this is just silly. What we need is “health care payment reform”.
There is probably an answer, but it is complex and won’t fit in a few paragraphs.
Overall, we are operating a health care system as a for-profit enterprise (yes, even the “non-profits” who are racking in a lot of money that goes to compensation…they aren’t doing it for the love of people). That alone should tell you we are running down the wrong path. We have romantic notions about competition, but when you take the time to think where and how that competition is supposed to take place, it doesn’t take long to realize that this notion is as naive as believing in Santa Claus.
As dianne pointed out above:
1. There are multiple sets of prices. There is list price which is what they will (and do) charge anyone unlucky enough to not have a coupon…er, insurance. Just because most people don’t pay that price doesn’t mean no one pays that price. Again, this is for health care.
2. The insurance system (created due to increasing greed by doctors and hospitals originally) has created nothing but waste.as the insurance companies try to out-greed the others. This is nothing more than pure waste that should be spent for…wait for it…health care.
3. The most nauseating aspect of our current system that points right back to money being the prime motivator. They simply don’t care about the subscribers.
TL;DR -- follow the money; there is a lot of greed going on by people who have no empathy for their fellow humans
Fire all the healthcare CEOs and strike their profit motive…I’m sure that’s not the entire picture but every dollar that goes to profit is one that didn’t go to patient care. For profit health care has a perverse incentive scheme from the get go. It’s not like there is competition to speak of, at best most markets are oligopolies and the majority of (R) controlled States have 1 for profit provider. Monopolies are known for their efficiency and high quality products? There have even been pushes for FEDGOV legislation to let those single State monopolies merge across State boarders to create even bigger monopolies.
Also, as an atheist, I’m very annoyed when health insurance companies refer to the number of ‘souls’ in their care.
We have romantic notions about competition, but when you take the time to think where and how that competition is supposed to take place, it doesn’t take long to realize that this notion is as naive as believing in Santa Claus.
It’s even worse than you think. There are several problems here.
First, how can competition work when the customer has no way of judging the quality of the product? The average person is going to have great difficulty sorting out whether his or her health care provider is the best choice or even competent. Whether the person’s outcomes are good or not? Maybe, but if you use that metric some hospitals will brag about their wonderful outcomes and keep those outcomes good by refusing anyone who is even slightly high risk. (For example, hospitals with low c-section rates that refer out any woman with a history of a c-section, macrosomy, twins, etc.) How good their bedside manner is or how nice the staff are? Studies have suggested that facilities that do well on these metrics may actually be providing worse care than those that do worse. So it becomes about reputation, trust, and a whole lot of unverified guessing.
Second, how often is there any actual choice? Insurance, especially HMOs, drastically reduce patients’ options for everything from which provider to go to to which lab to use. And how do you make an informed choice about which hospital to go to while you’re in labor or bleeding to death or having a heart attack? The only reasonable choice in an emergency is the nearest. (Not to mention people who live in remote areas with only one hospital within 100 square miles or so…)
Third, even if there are choices available, who chooses their doctor based on price? My first question is whether they are any good or not. Ok, realistically, my first question is usually do they have an opening? It’s harder to get an appointment in the US than the propaganda would have you believe. So there’s little or no incentive to decrease price.
Fourth, there’s price fixing involved. Medicare says what they’ll pay. Other insurers follow suit. Hospitals charge what they can. Again, no motivation for decreasing price. No insurer will pay more or a larger percentage.
I have heard of “cash only” practices which do provide services at a lower rate in return for being paid cash up front and having the customer then negotiate with the insurance company him or herself. That’s probably fine for essentially healthy people, but who has a spare $100K lying around to pay cash for a hospitalization? So, not a workable model for the major part of the industry.
The employer-based health care system is totally insane. What is even more insane is that so many people here think that it is so great that they are frothing mad at the thought of a single-payer alternative. Except when they get old and use Medicare, which they love and seem to forget forget that it is exactly the system they hate most. I simply cannot understand how their minds work.
I’m pretty sure that’s the problem right there, their minds aren’t working. 🙂
I often wonder, too, at the inability to recognize that highly-educated people are able to have the information to make choices about their health care, and do so by not moving to the United States, where their health care becomes at the whim of their employer, rather than being a basic human right. There just can’t be any health care system that is better for having the profit motive be the major driving factor ahead of patient outcomes. The US has become a place where the unfettered market has been tried, and it’s proving to be a complete bust in many different ways: the only thing the Invisible Hand is giving 99% of the world is the Invisible Middle Finger.
Introducing competition into the NHS (UK) does not seem to have produced great benefits apart from a doubling of the salaries of GP’s. On the subject of American socialized medicine phobia -- this is from a 2009 Register article:
Investor’s Business Daily editorial :”The controlling of medical costs in countries such as Britain through rationing, and the health consequences thereof, are legendary. The stories of people dying on a waiting list or being denied altogether read like a horror script: People such as scientist Stephen Hawking wouldn’t have a chance in the UK, where the National Health Service would say the life of this brilliant man, because of his physical handicaps, is essentially worthless.”
The paper has since been notified that Hawking is both British and still among the living. And it has edited the editorial, acknowledging that the original version incorrectly represented the whereabouts of perhaps the world’s most famous scientific mind. But it has not acknowledged that its mention of Hawking misrepresented the NHS as well.
“I wouldn’t be here today if it were not for the NHS,” Hawking told The Guardian. “I have received a large amount of high-quality treatment without which I would not have survived.”
These arguments strike me as essentially the same ones I heard 25-30 years ago about the Canadian health care system (I had a fair amount of Canadian relatives).
Then, a few years later, these complaints were the same as actual news stories about the various problems with HMOs in the U.S.
Since then, access to, and cost of, healthcare has just continued to climb out of reach for more and more people.
Every day, in every hospital, people are admitted for expensive procedures that could have been (relatively) easily and cheaply prevented if there was universal access to affordable care and preventative treatment. but apparently that’s crazy-talk.
A socialized take on healthcare/health insurance just makes so much more sense to me. Almost everyone is going to need some degree of health care during their life. We may not be able to accurately predict any individual’s needed treatment and the resulting costs, but we can quite accurately make the prediction of the treatments/costs of, say, 100K people. I think the most reasonable thing to do is to take the amount of money necessary for that treatment, add enough to cover administrative/overhead expenses, maybe add a buffer (10%? I don’t have any clue…), spread the cost, and bank it in various investment formats. I may be over-simplifying it, as health care and economics is far from my specialty, but I’m not sure how such a plan could be horrible. Adding a profit margin into the mix only makes it more costly, and less efficient at best (and, as we see in the U.S. system, ultimately detrimental…).
I know Chris Hedges isn’t real popular amongst some of the atheist crowd (and I can’t find the particular section with my meager googling), but I thought he had a really good bit about governments controlling/supplying things that had a moral aspect to them. so, like, it’s perfectly cool to let the free market handle things like, say, action movies, key chains, and french fries, but something like car safety regulations, health care, and education should most definitely have government involvement. (I’m pretty sure I mangled even a poor paraphrasing of that…)
The employer based system is an historical relic. During WWII wages were capped. Benefits weren’t. So companies started to compete for scarce workers by offering additional benefits like health care. That proved to be popular and was expanded after the war. At that time it wasn’t a bad thing, but it should have long since been replaced by a real health care system.
I like chris Hedges and if you search for his name on my blog search window you will find many favorable mentions, especially at the time of the Occupy movement. Sure he is not an atheist but he has been a solidly progressive voice on so many things.
Sorry Mano, but this is totally off. As multiple commenters above have pointed out, no one actually pays these prices, except if they’re uninsured (and have enough assets for the hospital to pursue). This is what made the meat of Brill’s article, but still misses the point. Chargemaster costs are not the cause of excess costs because the majority of payers only pay a fraction of those costs.
If you want to read actual research into excess costs of US medical care I would recommend starting with the 2008 McKinsey report on excess costs.
Articles and graphics like these provide a knee-jerk, and emotional reaction but are actually responsible for actively misinforming people about what the real problems are. I’ve been writing about the excess cost issue for years, and this is one of the most common errors people make. It’s not the charges, if anything it’s the stupid fighting over the charges requiring double the administrative costs.